Neurodiversity

What is Neurodiversity?
Neurodiversity describes the idea that people experience and interact with the world around them in different ways. One’s style of neurocognitive functioning can be Neurotypical or Neurodivergent. There is no right way of thinking, learning, or behaving. Differences are not deficits but expressions of our human diversity. Today, this paradigm includes people with ADHD, Learning Disorders, Tourette’s, and Autism. Neurodiversity promotes social justice for people who are not neurotypical. Incorporation of a neurodiverse perspective creates a strengths-based framework for those working with and serving autistic individuals.
Key Terminology in Neurodiversity
Neurodiversity is the variation in neurocognitive functioning species. Individuals are neurodiverse. Click here for a link with up-to-date, culturally competent terms.
Key Concepts of Neurodiversity
Key concepts
Social Disability: Disability does not create limitations, the environment’s failure to accommodate does. Neurodivergent individuals can contribute to society based on their unique strengths and abilities despite nonconformity to societal expectations.
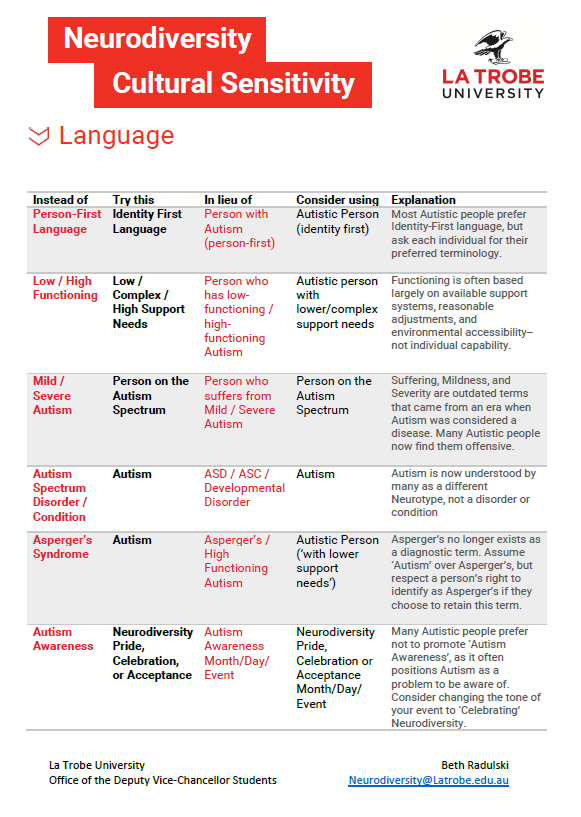
Autism and Self-Identity: A person is autistic, not someone with autism. People in the autistic community often prefer to use “identity-first” language (e.g., “an autistic woman”). Historically, person-first language has been used (e.g. “a woman with autism”). It’s important to honor everyone’s preferences. Consider asking each client, “How would you like me to address you?”
Cultural Perspectives: Human competence is defined by the cultures to which you belong. Industrialized cultures may value workers with advanced social, verbal and logical skills. Visual thinkers and “hands on” workers may experience more barriers in these societies. Temple Grandin speaks cogently about these issues in her numerous books.
Camouflaging (autistic or social masking):Autistic people may camouflage their innate autistic social behaviors to “fit” into a predominantly neurotypical social setting. Females, who tend to be diagnosed later in life, report that social masking requires exceptional effort. This can result in “autistic burnout”, frequently misconstrued as depression, anxiety, mood lability, or social isolation.
Gender identity: Neurodivergent individuals, particularly those with autism, are more likely to identify as gender diverse (including transgender, nonbinary, genderqueer, etc.) than neurotypical individuals. Ask patients about their preferred pronouns as well as gender dysphoria.
How has Neurodiversity Influenced Autism Diagnosis and Treatment?
DSM clinical criteria for autism has changed significantly in the past 75 years. “Autism” was derived from the Greek term “autos” (“self” ) to describe a “state of detachment from reality when the inner life of a patient becomes predominant.” Eugen Bleuler, a Swiss psychiatrist who studied schizophrenia, created the term in 1911. DSM I (1952) defined “autism” as “schizophrenic reactions prior to puberty.” DSM III (1980) recognized “autism” as distinct from childhood schizophrenia. DSM IV (1944) noted autism as a spectrum disorder. Neurodiversity was conceptualized by Judy Singer, Australian sociologist, in 1998. She launched the neurodiversity movement as an outgrowth of the autism and wider disability rights and advocacy movement. Additionally, autistic adults have created community on the Internet, sharing common experiences of self-identity and empowering communication. This has led to a distinct autistic culture. This movement is currently shaping DSM 6 revision for Autism diagnosis. Also note, DSM-5 (2013) dropped using “Asperger’s” to designate high functioning autism due to Dr. Asperger’s Nazi involvement of identifying “unfit” children for elimination.
DSM 6 (2027) will incorporate the values of the Neurodiversity movement with refined focus on inclusivity, cultural competence, individual variation, and personalized treatment. Since the 1990s, adult activists of the Neurodiversity Movement have assisted parental advocates to seek legalized rights, educational accommodations, federal funding for research, and services for their family members.
Autism Controversies and Concerns
Autism Controversies and Concerns
Eugenic policies in the 1900s encouraged institutionalization and sterilization of youth consider “feeble-minded” as it was believed the condition was inherited. Influential researchers in the 1940s were Hans Asperger who studied high functioning male youth and Leo Kanner who believed “refrigerator moms”/“cold” parenting was causative. By the 1960s, Bernard Rimbland argued for biological causation. He established the National Society for the Autistic Children (Autism Society of America). In the 1970s, the term developmental disability was legally introduced, Courts granted rights to school attendance for developmentally disabled children and the Education for All Handicapped Children Act was passed. Subsequent laws have included Individuals with Disabilities Education Act (1990), Combatting Autism Act (2006), Autism CARES (Collaboration, Accountability, Research, Education, and Support) Act ( 2014, 2024).
Wakefield (Lancet 1998, 2002) proposed an etiologic link to MMR vaccines. Subsequent research disproved this with a formal retraction in 2010. In 2025, Robert Kennedy Jr (HHS) has shifted federal focus on vaccine skepticism and will direct new research efforts in this direction. The Trump administration’s current defunding of education and DEI initiatives will significantly impact rights.
Screening for Autism
Primary care providers can use primary Autism screening tools. Our DocAssist website offers links and more information related to the M-CHAT-R/F Modified Checklist for Autism in Toddlers, Revised with Follow up and the CARS2 – Childhood Autism Rating Scale.
Specialized clinicians may further evaluate using the following screening tools:
SWYC- Survey of Well-being of Young Children (SWYC)
POSI- Parents’ Observation of Social Interaction
CSBS-ITC- Communication and Symbolic Behavior Scales Developmental Profile – Infant-Toddler Checklist
SCQ- Social Communication Questionnaire
STAT- Screening Tool for Autism in Toddlers & Young Children)
SRS – Social Responsiveness Scale
How to use the Neurodiversity Framework in your Practice
Help parents appreciate the unique strengths of their child whether they are neurotypical or not. Think about how you approach discussing temperament, body type, artistic or athletic skills, gender identification, and sexual orientation. Humans are diverse. Model positivity and acceptance and lack of stigma, use the term autism, ADHD, dyslexia, etc. Offer hope and connect patients to specialists, support groups, resources and services when indicated.
Resources
Click here to learn more on how to make your office setting more comfortable for autistic patients.
Click here for access to Dr. Charney’s Webinar, Caring for Youth with ASD/IDD in Medical Settings.
Click here for access to Dr. Charney’s Webinar Evaluating Behavioral and Psychiatric Symptoms in Youth with ASD/IDD.
Click here for access to Dr. Charney’s Webinar Using Psychotropic Medications in Youth with ASD/IDD.
Learn more about the history and timeline of Autism.
Finally, educate yourself with this recommended book list:
1. Differently Wired: Raising an Exceptional Child in a Conventional World by Deborah Reber
2. Neurotribes by Steve Silberman
3. Autistic Community and the Neurodiversity Movement by Steven Kapp
4. Books and videos by Temple Grandin
5. Unmasking Autism: Discovering the New Faces of Neurodiversity by Devon Price
6. The Real Experts: Readings for Parents of Autistic Children by Michelle Sutton
7. Autism in those Socialized as Girls/Women: Hidden for Too Long
8. Autism- It’s Different in Girls
9. ‘Social Camouflage’ May Lead to Underdiagnosis of Autism in Girls